
A report released today stated that 43% of Australians received sub-standard (below best practice) care at each visit to a general practitioner. http://www.abc.net.au/news/2012-07-16/healthcare-system-failing-australians/4132056. Apparently this is largely due to GPs not being up to date with the latest treatments and practices. Smart phones were suggested as a way to improve the situation.
I recently spent a couple of weeks in Africa looking at ways to increase the effectiveness and reach of mHealth initiatives. Its customary to emphasise the importance of low cost devices in developing countries. Applications that only require SMS or voice can be used by the widest number of people on the lowest cost phones with the longest battery life. Which is absolutely true if you are creating an application to be used by the general population or community health workers then this is almost certainly the sort of phone technology that should be your first preference. To some extent this is also still true in developed countries. If SMS works for your app then you should probably use it.
However I think you can make a strong case that doctors in developing countries can benefit just as much from smart phones as GPs in developed countries, if not more so. Just as mobile phones leap frogged land lines, supplying a developing country doctor with a smart phone or tablet connected to a cloud based server can be much simpler than equipping the clinic with PCs and associated medical software. It is also cost effective if that phone becomes an integral part of treating scores of patients per day and reporting health informatics.
The following diagram attempts to illustrates this.
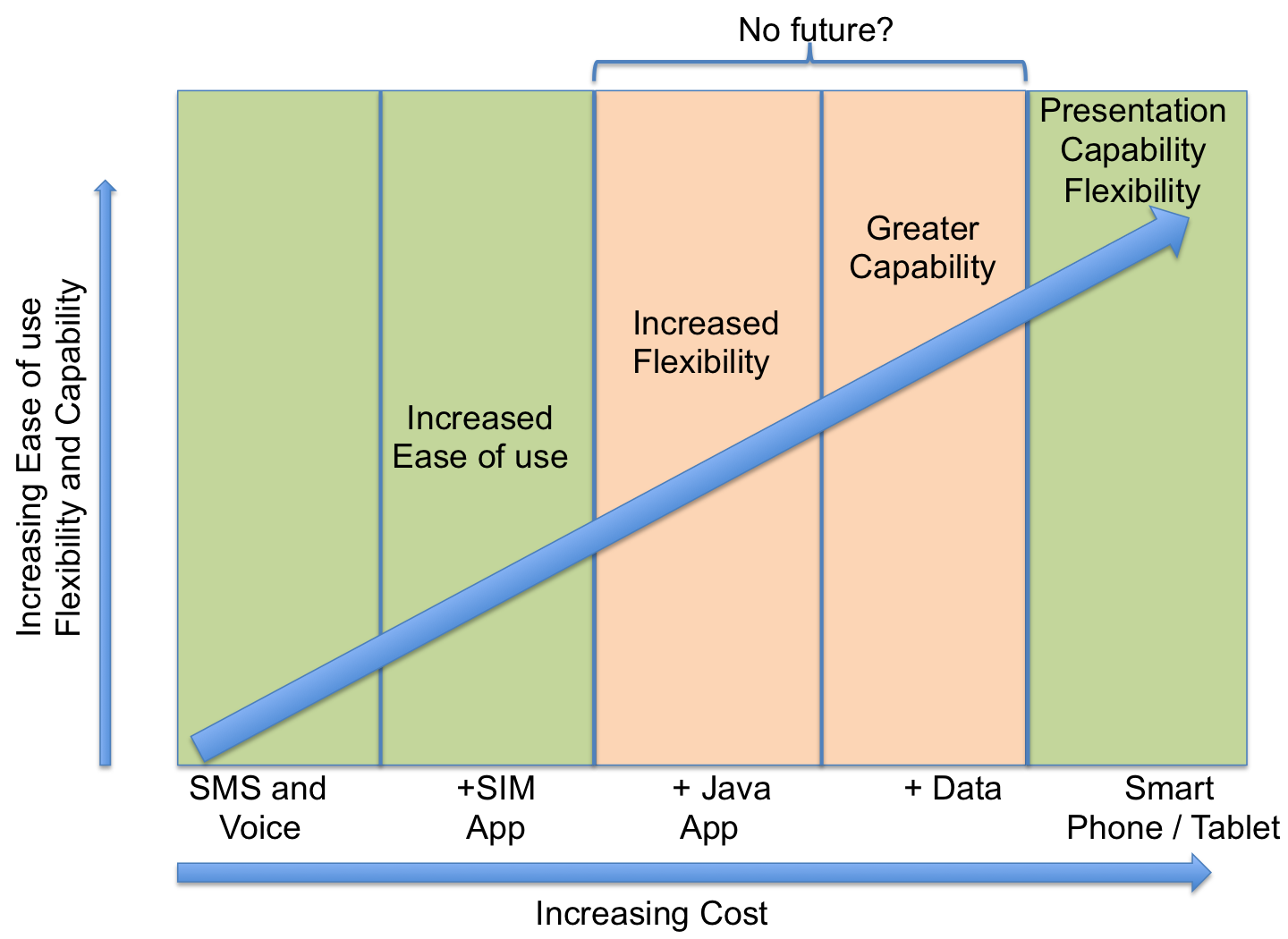
No future for j2me phones? There does not seem to be much development happening on these phones in developed countries nowadays. I don’t think that it should be so different in developing countries. So maybe applications should either be aimed at low cost devices over SMS / Voice, or smart phones, or both.
Hi Neil,
It was a pleasure meeting you in Kenya, and this is an interesting diagram. My rule of thumb with ICT projects in Africa is that if a smartphone can displace a computer, you should definitely do so because the smart phone is cheaper, more familiar to your users, and is more resilient (durability and battery life). When people ask me to do something with a smart phone that they wouldn’t do with a computer, I ask whether they really just want simple phone functionality and might be able to make do with a SIM app.
I agree there’s something of a no-man’s-land around j2me, and it’s partly due to the capability/cost ratio. It also has to do with the fact that j2me is a fractured standard – you almost never find a j2me app that just works and looks the same on every j2me phone. A similar conversation is happening on the smart phone side – should we develop just once for a browser, or instead focus on specific smart phone OS? Right now apps have more capabilities but there are tools to build mobile browser-based apps that function like a native app (i.e. are usable when offline). At Medic Mobile we’re betting on the Internet – browsers – rather than app platforms. This mainly has to do with smart phones but there is some potential to spill over into feature phones with browsers like opera – this jquery diagram has some food for thought. http://mxlbs.de/en/jquery-mobile
Hi Isaac,
Its good to hear from you again. I agree with you. My intention is to make sure that any administrative or analytic component of the Smap application has be able to be used from a mobile phone and JQuery Mobile is one of the tools we are using to do that.
We have also been using “Phone Gap” for those components that need to access hardware such as the gps, accelerometer etc. For us these are the survey client apps.
Hi Neil,
I can’t talk to the J2ME debate, it is clear that there is potential for both developing and developed counrties in the use of mobile devices for data and information to improve systems and services. The problem with many developed countries is the legacy systems and “territory” battles that happen within Govt minitstries, particularly the health service. Having used the UK health service over the past few years, there is jawdropping inefficiency in the way it works that moving onto mobile and electronic based systems would have a large impact on.
I agree with Isaac, that essentially where many of us thought the next phase of the web globally was around speed, it is actually about mobility. In terms of developing countries, I think that we have all been taken by surprise by the impact of mobile phones. I was recently at the Pacific Health Summit http://www.pacifichealthsummit.org/policylabs/affordabletech/innovation.aspx where there was a lot of encouraging evidence of mobile and e-medicine taking off in a number of developing countries. The key thought that I took away from the conference is that there is much that developed countries can learn from developing countries when it comes to innovation in mobile and e-products for health. So, Neil, I think your thinking is in the right direction.